
CoreHealth came to us in July 2023 with a brief that most development companies would have turned down.
Their major client needed a fully functional doctor consultation platform. The previous contractor had left behind a legacy codebase that was outdated and impossible to integrate with modern tools. CoreHealth had 6 weeks. Their budget was tight. The platform needed to connect with multiple third-party systems from day one.
We took the project. We delivered in 6 weeks. And what started as a single MVP became 3 separate telemedicine products over the following year.
Here's what happened, and what it took.
The brief was brutal
In England, 1 in 10 people wait more than 3 weeks to see a general practitioner. For CoreHealth, a UK healthtech company that has been building telemedicine platforms since 2006, that gap is the business case. Every week a platform is delayed is a week patients wait longer for care they need.
So when CoreHealth's major client needed their consultation platform modernized, CoreHealth gave themselves 1.5 months. No buffer.
The technical situation made it harder. The platform had been built by a previous contractor and couldn't support modern integrations. A full rewrite was necessary, not a patch job. The budget didn't allow for a large team or a slow start.
We were the development partner CoreHealth chose to get it done.
Why most teams miss these deadlines
The industry average for a comparable telemedicine MVP is 4 to 6 months. Some teams take longer.
That's usually a process problem, not a technology problem.
Large teams create coordination overhead. When 10 or 12 people are building the same platform, handoffs multiply, decisions slow down, and meetings become the most productive thing happening. Speed goes down as headcount goes up.
Skipping discovery to save time creates scope drift. A team that starts coding before mapping every user flow and integration point will hit blockers mid-build. Those blockers cost more time to fix than a proper discovery phase would have taken. Integrations are the most common culprit: when video calling, scheduling, prescription management, and pharmacy fulfillment all need to talk to each other, planning them as an afterthought is expensive.
Stack choices compound the problem. A monolithic backend not designed for API-heavy workflows turns every new integration into a retrofit. The first integration takes a week. The fifth takes three.
What we did differently
We put 5 people on the CoreHealth project: 1 frontend developer, 1 backend developer, 1 QA engineer, 1 UI/UX designer, and a project manager. Each person owned a lane. No overlap, no ambiguity about who was responsible for what.
Before any development started, we ran discovery. That meant reviewing the existing application to find every technical and logical gap across all user flows, then decomposing the platform into functional modules. Deliverables: Q&A documentation, user story documentation, a project estimation and roadmap, a low-fidelity prototype, and completed UI/UX design. All of that before a single line of production code.
For the stack, we chose React.js on the frontend and Node.js on the backend. The platform needed multiple third-party integrations from day one, and this stack is well-suited for API-heavy architectures. It also let us build fast without cutting corners on quality.
We also work with AI-augmented workflows across coding, project management, QA, and CI/CD. Our architects own the structure and the long-term decisions. AI handles the repetitive implementation work. A 5-person team working this way builds at a pace a traditional 10-person team often doesn't reach, because administrative overhead drops out of the process entirely.
The 6-week process
Here's how the delivery broke down:
| Phase | Month |
|---|---|
| Discovery | July 2023 |
| UI/UX design | August 2023 |
| Development | September 2023 |
| MVP delivery | October 2023 |
| Further collaboration | November 2023 |
| Ongoing | December 2023–2024 |
Team allocation across phases:
| Role | Discovery | Development |
|---|---|---|
| Frontend developer | Full-time | Full-time |
| Backend developer | Full-time | Full-time |
| UI/UX designer | Full-time | Full-time |
| QA engineer | Full-time | Part-time |
| Project manager | Full-time | Full-time |
Step 1: Discovery
We reviewed the entire application and mapped technical and logical gaps across every user flow. Then we applied feature-based decomposition, breaking the platform into modules that could be built and tested independently. By the end of discovery, we had Q&A docs, user story documentation, a project estimation, a roadmap, a low-fidelity prototype, and completed UI/UX design.
This is the phase where deadlines are saved or lost. Teams that skip it to move faster run into integration blockers and scope drift mid-build. Those problems cost more to fix than the discovery phase would have taken.
Step 2: Design
Using the discovery artefacts, we refined the prototype through a client feedback loop before moving to development. The goal was an interface that was clear and build-ready, with no rework needed once coding started.
Step 3: Development
The full team built the frontend in React and the backend in Node. External integrations were scoped and built from the start, not added after the fact. QA ran part-time in parallel, catching issues as they were introduced rather than in a testing sprint at the end.
Step 4: Delivery
We delivered the MVP on time. CoreHealth presented it to their client. The response was exactly what they'd hoped for.
The relationship didn't end there. Read the full case study
What the MVP became
That first delivery opened a door.
The architecture we built wasn't scoped for one use case. It was designed for the complexity CoreHealth operates in. Over the following months, it expanded into 3 distinct telemedicine products.
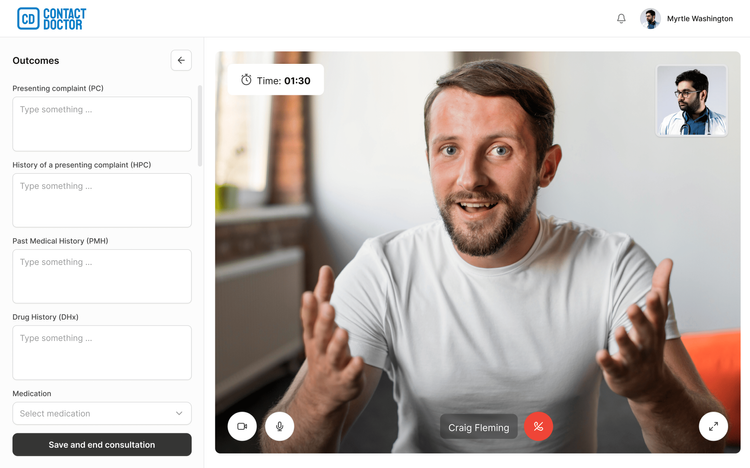
Doctor consultation platform
Patients book consultations online, browse doctors by specialty, and pick time slots that fit their schedule. The platform supports real-time video consultations and secure data handling for both patients and providers.
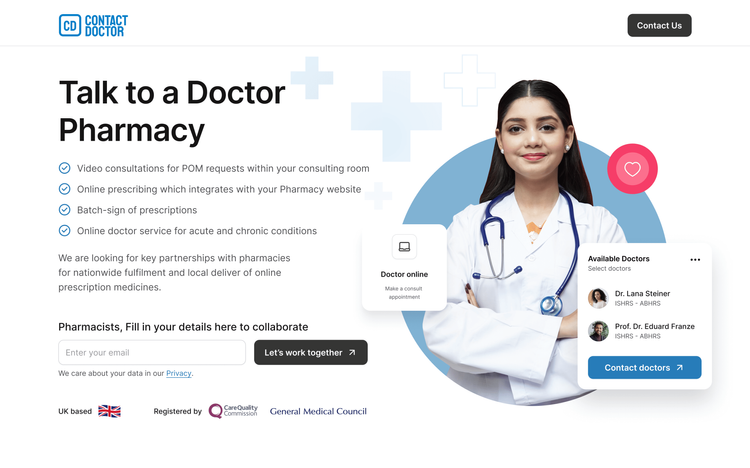
SaaS platform for pharmacies
Built for pharmacies offering online prescription services. Patients consult with licensed doctors by video, and if a prescription is approved, it goes directly to the pharmacy for immediate collection. For cases that don't require a live session, patients can complete a medical form online instead.
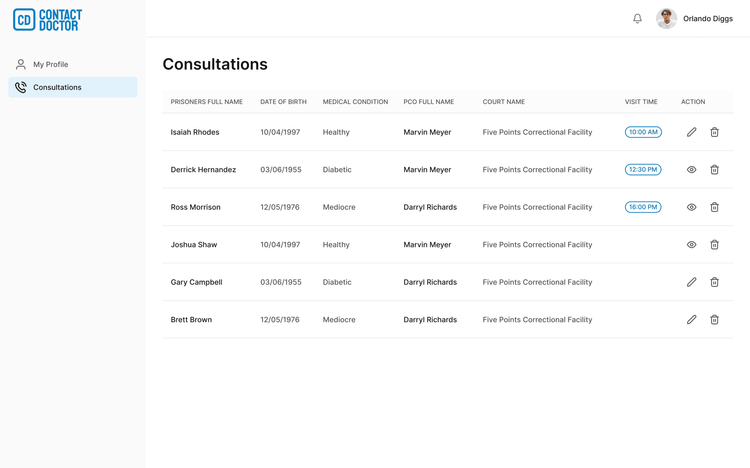
Healthcare platform for prisons
A secure telemedicine solution compatible with Samsung Tab A8 tablets. Prisoners consult with healthcare providers directly from their cells. When a physical assessment is needed, providers can conduct it remotely via the tablet camera.
All 3 products share the same core architecture from the original 6-week MVP. That wasn't a coincidence. It's what a discovery-first, integration-ready build makes possible.
| Before | After |
|---|---|
| Legacy codebase | Modern, maintainable codebase |
| 1.5-month hard deadline | MVP delivered in 6 weeks |
| No external integrations | Multiple third-party integrations live from day one |

What this tells you about telemedicine software development
A few things from this project are worth naming, because they run counter to how many teams approach healthcare builds.
Discovery is the phase that makes everything else go faster. Every hour spent mapping user flows and decomposing features saves 2 to 3 hours of rework in development. Teams that skip it in the name of speed end up losing more time than they saved.
Your stack choice is an integration decision. Telemedicine platforms talk to a lot of systems: video APIs, booking tools, pharmacy management, EHR systems, payment processors. React and Node work well here because the JavaScript ecosystem is built for API-heavy applications. There are other valid choices, but the tradeoffs are real and worth thinking through before you start building.
Team completeness beats team size. 5 people who each own a defined lane move faster than 12 people with overlapping responsibilities. Communication overhead grows with every person you add to a project. For a well-scoped MVP, a lean, complete team will consistently outpace a larger one.
Compliance belongs in week 1. In the US, HIPAA compliance typically adds $15,000 to $50,000 to a healthcare build, covering encrypted storage, access controls, and penetration testing. In the UK and EU, the relevant frameworks are GDPR and CQC standards. Either way, building compliance into the architecture from the start costs significantly less than retrofitting it later.
You can also see how this approach plays out across other industries in our case studies.
How to plan your telemedicine MVP
Start with your integrations. List every external system your platform needs to connect to: video calling, appointment scheduling, EHR or patient records, pharmacy systems, payment processing. This list determines your stack and your timeline more than any other single factor.
Know what discovery should produce. A real discovery phase delivers user stories broken down by role (patient, doctor, admin), feature decomposition by module, a low-fidelity prototype reviewed with your end-user or client, and a project estimation with a roadmap. If a development partner doesn't produce these before they start building, that's worth asking about.
Minimum viable team for a telemedicine MVP:
| Role | Allocation |
|---|---|
| Frontend developer | Full-time |
| Backend developer | Full-time |
| UI/UX designer | Full-time |
| QA engineer | Part-time |
| Project manager | Full-time |
Set realistic timeline expectations. A focused MVP with well-defined scope can ship in 6 to 10 weeks. Every integration added after the build starts costs 2 to 4 additional weeks. The scope you lock in during discovery is the scope you'll ship.
Plan compliance before architecture. HIPAA in the US, GDPR and CQC in the UK and EU. Designing for it from week 1 costs less than building it in after the fact.
If you're still evaluating development partners, our guide to top MVP development companies covers what to look for and how to compare.
Want to talk through what your telemedicine build would actually involve? Get in touch and we'll give you an honest estimate.
Frequently Asked Questions
A focused MVP with defined scope can be delivered in 6 to 10 weeks. The CoreHealth MVP was delivered in 6 weeks by a 5-person team following a discovery-first process. Most mid-market telemedicine platforms take 5 to 7 months, largely because teams add scope during development or skip the discovery phase. Both of those things push integration work into the build and cause delays.
A basic telemedicine MVP with video consultations, scheduling, and secure data handling typically starts at $30,000 to $60,000. A mid-range custom platform with EHR integration, multi-role access, and prescription workflows costs $70,000 to $150,000 and takes 5 to 7 months. Enterprise platforms with AI features, IoT integration, and complex analytics run $300,000 and above. Eastern European development teams typically charge $20 to $80 per hour, which is 40 to 60% less than US rates for comparable experience.
Core features for most telemedicine platforms:
- Patient registration and profile management
- Doctor profiles with specialty filtering
- Appointment booking and scheduling
- Real-time video consultations (via WebRTC, Twilio, or Agora)
- Secure messaging
- Prescription management
- Medical record access and upload
- Admin dashboard for clinic or platform management The right feature set depends on the use case. A pharmacy prescription platform needs different workflows than a general consultation platform or a prison healthcare system.
React and Node.js is a strong choice for telemedicine platforms that need multiple third-party integrations. The JavaScript ecosystem is built for API-heavy systems, and using the same language across frontend and backend reduces context-switching for the development team. For mobile, React Native offers cross-platform delivery from a shared codebase. Video is typically handled via WebRTC-based solutions or third-party services like Twilio or Agora. The best stack depends on your integration requirements, not just your performance goals.
If your platform handles protected health information (PHI) for patients in the United States, HIPAA compliance is legally required. This covers encrypted data storage, strict access controls, audit logs, and Business Associate Agreements with every vendor handling patient data. Budget $15,000 to $50,000 for the compliance architecture and third-party security testing. In the UK and EU, the relevant frameworks are GDPR and CQC standards. Plan for compliance before your architecture is designed.
The CoreHealth platform was built by 5 people: 1 frontend developer, 1 backend developer, 1 QA engineer, 1 UI/UX designer, and a project manager. This is the minimum viable team for a focused MVP. Each person owned a defined domain with no overlap. Larger teams aren't faster unless the scope genuinely requires parallel workstreams. For a well-scoped MVP, a lean, complete team will outpace a larger one.
Off-the-shelf platforms like Teladoc or Doxy.me make sense for standard use cases: basic video consultations, simple scheduling, one patient type. They're faster to deploy and cheaper upfront. Custom development is the right call when your platform needs unusual integrations, serves a specialized patient group, or will become a product you sell to other organizations. CoreHealth needed a white-label platform their own clients could use, so custom was the only viable path. The decision comes down to whether your requirements fit the off-the-shelf product, or whether the product needs to fit your requirements.